
Gavi and Cochrane are lying about the efficacy and safety of HPV vaccines
By Dr G Delépine, a cancer surgeon and statistician
The Cochrane Collaboration used to be the model of an organisation whose rigorous meta-analyses objectively summarised the current state of medical knowledge. Its conclusions frequently contradicted the propaganda lies spread by Gavi and Bill Gates. The Bill Gates Foundation then awarded a “donation” of $1.15 million to the organisation [1] which subsequently expelled Peter Gøtzsche, who was regarded as too critical[2]. And ever since that donation, Cochrane’s publications have been bowing to Gates’s wishes, as in one of its most recent meta-analyses, which claims that « The HPV vaccine is highly effective at preventing cervical cancer and does not cause any serious side effects »[3].
The Gavi Foundation knows no bounds when it comes to the sheer scale of its lies[4] since she claims on France 24[5] , Libération[6], Le Figaro [7]or by Luc Blanchot[8] that « The HPV vaccine has saved more than a million lives worldwide » without specifying either its sources or how this figure was arrived at.
It is therefore once again necessary to highlight the reality of this vaccine’s dismal results in the real world.
In 2025, there is absolutely no evidence that this vaccine has prevented a single case of cancer
No randomised trial has demonstrated any reduction in the incidence of cervical cancer among those who have been vaccinated; on the contrary, in the pivotal trials – the ones that led to the vaccines being authorised for marketing – women who were vaccinated at a later stage showed an increase in precancerous lesions. To claim the opposite, the reviewers excluded these women from the analysis, thereby completely violating the principle of the randomised trial and the integrity of their conclusion.
Nineteen years after it was first marketed, a vast number of publications by authors linked to the pharmaceutical industry or to organisations responsible for vaccination continue to claim that vaccination prevents cancer; however, a closer examination reveals that these claims are not based on real-world data from at-risk groups [9] but on unexposed or imaginary groups[10] based on mere estimates derived from biased simulations[11] based on false assumptions.
The unbelievable lie that 17 lives are saved for every 1,000 people vaccinated!
In its press release, Gavi claims that the HPV vaccine could prevent 17.4 deaths per 1,000 girls vaccinated. This claim is completely at odds with the official data.
Worldwide, average life expectancy is around 70 years, with an annual mortality rate from cervical cancer of around 2 per 100,000 [12] [13] [14]. Over a woman’s lifetime, the risk of dying from cervical cancer can therefore be estimated at 1.4 per 1,000 women [15] which is 12 times less than what Gavi claims the vaccine can prevent (17 per 1,000).
In Africa, the continent most affected by this cancer, the main causes of death are [16] malaria, HIV/AIDS, respiratory tract infections, diarrhoeal diseases, perinatal conditions, cardiovascular diseases, tuberculosis, ischaemic heart disease, measles and road traffic accidents. Only 20% of deaths are due to cancer[17] of which approximately 20% relate to cervical cancer[18] (representing 4% of overall mortality). In 2022, around 100,000 cases of invasive cervical cancer were recorded, and nearly 76,000 women died from the disease [19] across the 47 African states, whose combined population included 700 million women, or 1 in 10,000 women. For an average life expectancy of 60 years, lifetime mortality can be estimated at 6 per 1,000, which is three times less than what Gavi claims the vaccine can prevent.
How could a vaccine – even if it were completely effective – prevent 3 to 12 times more deaths than the mortality rate from the cancer it is supposed to combat?
Gavi appears to draw inspiration from the principles of Joseph Goebbels (Adolf Hitler’s Minister of Propaganda) « A lie: the bigger it is, the more people believe it » “A lie repeated a thousand times becomes the truth”.
The misinformation perpetuated by Gavi is perpetuated by the media, which consistently publishes press releases from the pharmaceutical industry without ever verifying the accuracy of the official data, thereby grossly violating the journalistic ethics set out in their charter[20].
HPV vaccines have failed to prevent cancer
In the absence of conclusive randomised trials, the effect of these vaccines can be assessed by examining trends in the incidence of cervical cancer as recorded in the cancer registries of countries that have made vaccination compulsory. These registers are maintained by officials who are independent of the pharmaceutical industry.
All the published data from these registries show that cytological screening has been followed everywhere by a reduction in the incidence of invasive cervical cancer of between 30% and 70%. And since the introduction of vaccination, the overall incidence has plateaued and is even often rising among vaccinated women who have reached the age at which cervical cancer typically occurs.
In Australia, The introduction of cervical screening in 1991 was followed by a fall in incidence of nearly 50% (from 13 in 1991 to 7 in 2006).
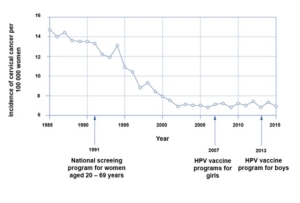
But the introduction of a school-based vaccination programme for 12- to 13-year-olds, with catch-up vaccinations available up to the age of 25[21] The programme, which began 19 years ago, has not succeeded in reducing the incidence across the entire population. In fact, it has increased in the control group of vaccinated women who have reached the age at which cancer typically develops (those aged 25 and over):

In the group of women vaccinated later in life (who were aged between 13 and 25 at the time of their Gardasil vaccination and aged 30–42 in 2023), the vaccination was followed by an even greater increase in incidence (50%).

This increase in incidence among vaccinated groups who have now reached the age at which cancer typically develops may partly explain the gradual slowdown in the decline in vaccination rates among those under 15 observed in Australia since 2020. The rise in incidence among vaccinated groups is all the more surprising given that, during this period, older women – who are not eligible for vaccination – have seen their risk of cancer fall sharply thanks to screening programmes: -30% (5.6 to 4) for those aged 60–64, -20% (6.5 to 5.1) for those aged 65–69, and -28% (5.3 to 3.8) for those aged 70–74.
In 2024, the Australian national agency estimated the number of new cases of cervical cancer at 1,030 (an increase of nearly 33% on the pre-vaccination figure) and its incidence at 7.1 per 100,000[22] (that is, 15% more than in France, where vaccination rates are low). How can anyone believe in the imminent eradication of cancer that Gardasil’s advocates are constantly promising across all media?[23] ?
Great Britain introduced the Gardasil school vaccination programme for girls in 2007. Eighteen years later, the incidence of cervical cancer has risen in the vaccinated control group (aged 25–34), whilst it continues to fall among women over 40 (who were not vaccinated).
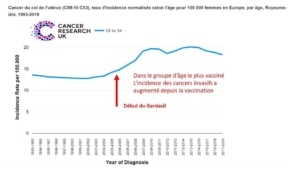
This rise in incidence among those who have been vaccinated casts serious doubt on the promise of the imminent eradication of this disease, as trumpeted by the vaccine advocates[24].
In Finland, The organised cervical cancer screening programme, which has been in place for over 30 years, has led to a 70–80 % reduction in the age-adjusted incidence of this cancer, as well as a reduction in mortality. However, Gardasil’s failure to prevent cancer has also been observed here.
In the group with the highest vaccination coverage that has now reached the age at which cancer typically develops (25–34-year-olds), the incidence of cervical cancer has risen by more than 70% (from 4.5 to 8).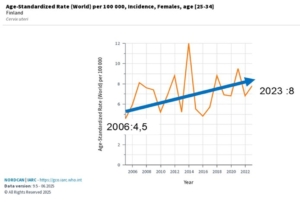
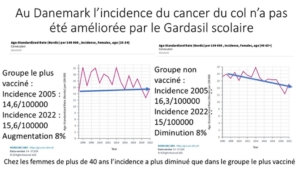
In Denmark
The vaccination of more than 85% young girls was followed by an 8% increase in the incidence of cervical cancer, whilst it fell by 8% among women over the age of 40 (unvaccinated).
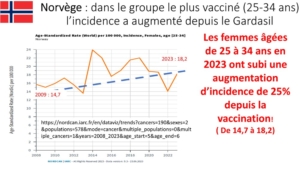
Gardasil’s ineffectiveness in preventing invasive cervical cancer has also been observed in Norway
Furthermore, anal cancer is observed almost exclusively in passive homosexual men and in immunocompromised individuals. Engaging in passive anal sex is the most significant causal factor and partly explains the consistently higher risk for women compared with heterosexual men (a 3- to 4-fold increased risk), and the 60 to 90 times higher risk among passive homosexual men, with an incidence of anal cancer of 95 per 100,000, rising to as high as 130 per 100,000 among those who are also HIV-positive. For a non-immunocompromised heterosexual man, the risk of anal cancer is virtually zero. Organ transplant recipients taking immunosuppressive drugs have an incidence of anal cancer five times higher than the general population, a rate similar to that of heterosexuals infected with the AIDS virus.
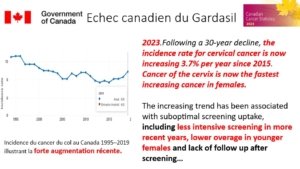
In Canada
Vaccination with Gardasil is also associated with an increase in the incidence of cervical cancer
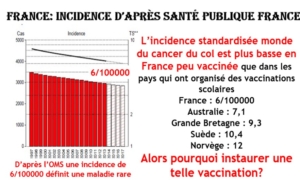
This stabilisation or increase in the incidence of invasive cancers in countries that have introduced widespread Gardasil vaccination stands in contrast to the steady decline in the incidence of cervical cancer in France, where officials nevertheless constantly lament our low vaccination rate.
In our country, where vaccination coverage is low, cervical cancer has become a rare disease – unlike in the countries with high vaccination rates that our leaders hold up as examples! And if we accept the new definition of eradication advocated by the WHO, we would even have eradicated it!
But it is true that, for the henchmen of Big Pharma and their shareholders, the only thing that matters is vaccinating everyone, regardless of the clinical results.
Gardasil is of no benefit to boys
To double the market for Gardasil, the vaccine has been promoted among boys on the pretext of preventing anal and throat cancers.
However, in France, anal canal cancer is very rare in men and does not therefore constitute a public health problem. In 2018, fewer than 400 cases were recorded in men, compared with the burden of prostate cancer (59,885 new cases in 2023) or lung cancer (33,438 men in 2023).
Furthermore, there is no evidence that Gardasil prevents this cancer.
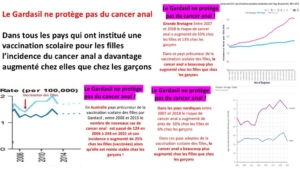
Data from national cancer registries show that, since the introduction of the school-based vaccination programme, there has been a greater increase in the incidence of anal cancer among girls – despite them having been vaccinated – than among boys.
Gavi and Cochrane are lying when they claim that vaccination with Gardasil is risk-free [25]
On Friday 27 October 2023, at Saint-Dominique Secondary School in Saint-Herblain, near Nantes, a Year 7 pupil died after receiving the Gardasil vaccine as part of the large-scale HPV vaccination campaign in secondary schools across France, initiated by President Macron. The Regional Health Agency was quick to assert that the vaccine was not to blame and dismissed any suggestion of organisational failings in the vaccination campaign.
Yet no one can deny that this child, who was in perfect health before the injection, died as a result of the school vaccination. But, as usual, the courts have not questioned the state’s responsibility for prescribing the vaccination, but only that of the scapegoat (the doctor), who now finds himself facing charges of manslaughter.
Unfortunately, this death following a Gardasil injection is not an isolated case.
In the US, according to the Vaccine Adverse Events Reporting System (VAERS), more than 400 deaths have been reported following Gardasil vaccination [26].
These deaths have led to numerous complaints in the US[27] cases occurring following Gardasil vaccination serve as a reminder that, during the clinical trials that preceded marketing authorisation, the mortality rate among those vaccinated stood at 8.5 per 10,000, which is nearly double the rate for women aged 15–24 in the general population of that age group. However, this was deemed a ‘coincidence’ by the pharmaceutical companies and the US Food and Drug Administration (FDA).
A critical review of these trials confirms a higher mortality rate among vaccinated women aged over 25, whose mortality rate was 2.36 times higher than in the placebo group. “When all the deaths among middle-aged women enrolled in the three trials are pooled, a higher case fatality rate was observed among those who received the HPV vaccine compared with those who received the placebo.” [28]
But the National Medicines Safety Agency claims that the mortality associated with Gardasil has spared the French (just as the agency responsible for nuclear safety had claimed that the Chernobyl cloud had spared France).
The Gardasil vaccine carries a risk of numerous other complications.
According to the National Vaccine Information Centre, tens of thousands of complications have been reported following Gardasil vaccination. The list of possible adverse events is, in fact, set out in detail in the CDC’s official publications [29]
and publications by The National Network for Immunisation[30].
Some very common complications are mild and temporary, such as pain at the injection site, oedema, swelling, fever, a cough, feeling unwell, hives, lymphadenopathy, epigastric pain, nasopharyngitis, headaches or nausea, sometimes accompanied by diarrhoea or vomiting.
Some are more severe, such as joint pain, arthritis, immune haemolytic anaemia, pancreatitis, hypothyroidism, syncope, muscle spasms, respiratory infection, gastroenteritis, appendicitis, urinary tract infection, postural orthostatic syndrome, thrombocytopenic purpura, systemic lupus erythematosus, myalgia, premature ovarian failure, infertility…
The most serious complications, which are fortunately very rare, such as Guillain-Barré syndrome, transverse myelitis, progressive encephalitis, pulmonary embolism, bronchospasm or an anaphylactic reaction, can be life-threatening. This is unacceptable for a treatment that is intended to be preventative for a disease for which a highly effective and completely risk-free method of prevention already exists (cytological screening).
According to figures from the US package leaflet for Gardasil, North American women are 100 times more likely to suffer a serious adverse event following vaccination with Gardasil than to develop cervical cancer. In particular, the risk of developing an autoimmune disease linked to Gardasil – even if the vaccine were effective – is far greater than the benefit of preventing a death from cervical cancer.
Are Gavi, Cochrane (since its takeover by Gates), the French Medicines Agency and the mainstream media deliberately lying, are they unaware of the English text in the US Gardasil package leaflet, or are they simply ignoring the CDC information that is inconvenient to them in order to claim that «Gardasil is safe»?
Doctors who administer the Gardasil vaccine risk legal action
The decision to place the French doctor who administered the fatal Gardasil vaccine to the child in Nantes under investigation is likely to be repeated in the event of the next vaccine-related incident, as the European Court of Justice recently ruled that « Doctors are solely responsible for the consequences of injections, as they are free to administer them, advise against them or refuse to do so ».
The Court even stated that «the’The marketing authorisation issued by the European Medicines Agency does not impose any obligation on doctors to prescribe and administer these vaccines to their patients’».
Doctors and other healthcare professionals who may administer Gardasil must therefore be particularly vigilant regarding the quality and comprehensiveness of the information provided to patients concerning the risks associated with the vaccine and the steps to be taken in the event of suspected adverse reactions. Even during an official vaccination campaign organised at school, they may be held liable.
As well as being ineffective and dangerous, Gardasil costs a fortune
In France, the flu vaccine costs between €6 and €11, the Sanofi Covid-19 vaccine costs €7.56, and the Infanrix Tetra® vaccine costs €14.63. A single dose of Gardasil is sold at a price of €116.83. This is an all-time record price for a vaccine. Depending on the age of the person being vaccinated, two or three doses are recommended. Taking into account the necessary medical consultations, HPV vaccination for an adult costs €500 and for a teenager around €350.
The cost of manufacturing a dose of Gardasil is estimated at less than $1 in Chaevia Clendinen’s thoroughly documented study [31], which states that « "The manufacturing costs of Gardasil sold to Gavi and developing countries range from $0.48 to $0.59 per dose."
Between 2006 and 2015, Merck generated nearly 14 billion dollars in sales of Gardasil; these then stabilised at 5–6 billion annually, bringing the total to nearly 40 billion dollars since the product was launched. According to some estimates, the Gardasil market is projected to be worth 46 billion USD in 2023. This colossal windfall provides a strong incentive for Merck’s shareholders to fund its propaganda and gives the company considerable resources to persuade political leaders and their advisers to promote Gardasil.
In the US, with 76 million children vaccinated at an average cost of $420 for the three-dose course, saving one American life from cervical cancer would cost around $18.3 million. By comparison, the value of a human life, according to the National Vaccine Injury Compensation Programme run by the Department of Health and Human Services (HHS), is $250,000 – the maximum amount the government programme awards in the event of a vaccine-related death.
In France, vaccinating an age group would cost nearly 300 million euros; that is to say, in the unlikely event of absolute efficacy, to prevent 1,000 deaths each year, a unit cost per life saved of 300,000 euros, which completely contradicts the public awareness campaign launched by Santé Publique France in 2019.
At a time when our finances and our hospitals are in such a dire state, the very idea of spending such a sum on Gardasil, given the unfavourable cost-benefit balance, is utterly scandalous.
[1] https://regisliber.wordpress.com/2020/05/14/pourquoi-la-fondation-gates-a-t-elle-rachete-cochrane/
[2] Peter Gotzsche, the man at the centre of the controversy
[3] Gabriela Galvin HPV vaccine: risk of cervical cancer falls, side effects minimal, according to a comprehensive review Euronews 24 November 2025
[4] https://www.gavi.org/fr/actualites/media-room/vaccin-contre-cancer-col-uterus-sauve-plus-dun-million-vies
[5] https://www.france24.com/fr/sant%C3%A9/20251116-cancer-col-uterus-vaccin-hpv-papillomavirus-sauve-un-million-de-vies-dans-pays-faible-revenus-gavi-deces
[6] ttps://www.liberation.fr/societe/sante/papillomavirus-plus-dun-million-de-vies-sauvees-grace-a-la-vaccination-dans-les-pays-pauvres-20251117_MU7Y5ILXCRHOJAQNA6RUGSTAHU/
[7] https://sante.lefigaro.fr/cancer-du-col-de-l-uterus-une-nouvelle-etude-de-reference-confirme-l-interet-du-vaccin-anti-hpv-20251124
[8]Cervical cancer: the HPV vaccine has saved over a million lives worldwide 18 November 2025
[9] As a recent Swedish article points out, which focuses on women aged between ten and thirty, whereas this type of cancer is usually only observed in women aged 25 and over
[10] https://www.courrierinternational.com/article/vaccination-laustralie-reve-deradiquer-le-cancer-du-col-de-luterus
[11]https://www.gyneco-online.com/gynecologie/elimination-du-cancer-du-col-en-australie-une-projection-pour-lavenir
[12] Boyle P, Ferlay J. Cancer incidence and mortality in Europe, 2004. Ann Oncol 2005 Mar;16(3):481–8.
[13] Ferlay J, Bray F, Sankila R, Parkin DM. EUCAN: Cancer Incidence, Mortality and Prevalence in the European Union 1998. 1999. IARC CancerBase No. 4, version 5.0. Lyon: IARC Press
[14] Remontet L, Esteve J, Bouvier AM, Grosclaude P, Launoy G, Menegoz F, et al. Cancer incidence and mortality in France over the period 1978–2000. Rev Epidemiol Sante Publique February 2003;51(1 Pt 1):3–30
[15] https://www.donneesmondiales.com/esperance-vie.php#google_vignette
[16] Read more: https://globometer.com/mortalite-deces-afrique.php
[17] https://www.insee.fr/fr/statistiques/2385258
[18] J.-C. Kajimina Katumbayi Epidemiological and histopathological characteristics of 1,280 cases of cervical cancer in Kinshasa https://www.sciencedirect.com/science/article/pii/S2468718921001860
[19] https://www.trtafrika.com/francais/article/18260132
[20]https://www.snj.fr/charte-dethique-professionnelle-des-journalistes/94
[21] https://www.health.gov.au/topics/immunisation/vaccines/human-papillomavirus-hpv-immunisation-service
[22] https://hpvcentre.net/statistics/reports/AUS_FS.pdf
[23]https://www.rtl.fr/actu/sante/papillomavirus-l-australie-en-passe-d-eradiquer-le-cancer-du-col-de-l-uterus-7794956907
[24] NHS England pledges to eliminate cervical cancer by 2040 https://www.bbc.com/news/health-67420138
[25] Martínez-Lavín M, Amezcua-Guerra L. Serious adverse events following HPV vaccination: a critical review of randomised trials and post-marketing case series. Clin Rheumatol. October 2017;36(10):2169–2178.
[26] https://vaers.hhs.gov/eSubDownload/index.jsp?fn=2025VAERSData.zip.
[27] https://www.wisnerbaum.com/prescription-drugs/gardasil-lawsuit/gardasil-deaths/
[28] https://pmc.ncbi.nlm.nih.gov/articles/PMC6494566/pdf/CD009069.pdf
[29] Human Papillomavirus (HPV) Vaccine Safety 6 March 2025 https://www.cdc.gov/vaccine-safety/vaccines/hpv.html
[30] https://immunizationinfo.com/gardasil-vaccine/
[31] Haevia Clendinen, Yapei Zhang, Rebecca N. Warburton, Donald W. Light, ‘Manufacturing costs of HPV vaccines for developing countries’, *Vaccine*, volume 34, no. 48, 21 November 2016, pp. 5984–5989.